
Disc Herniations (Slipped / Herniated Disc)
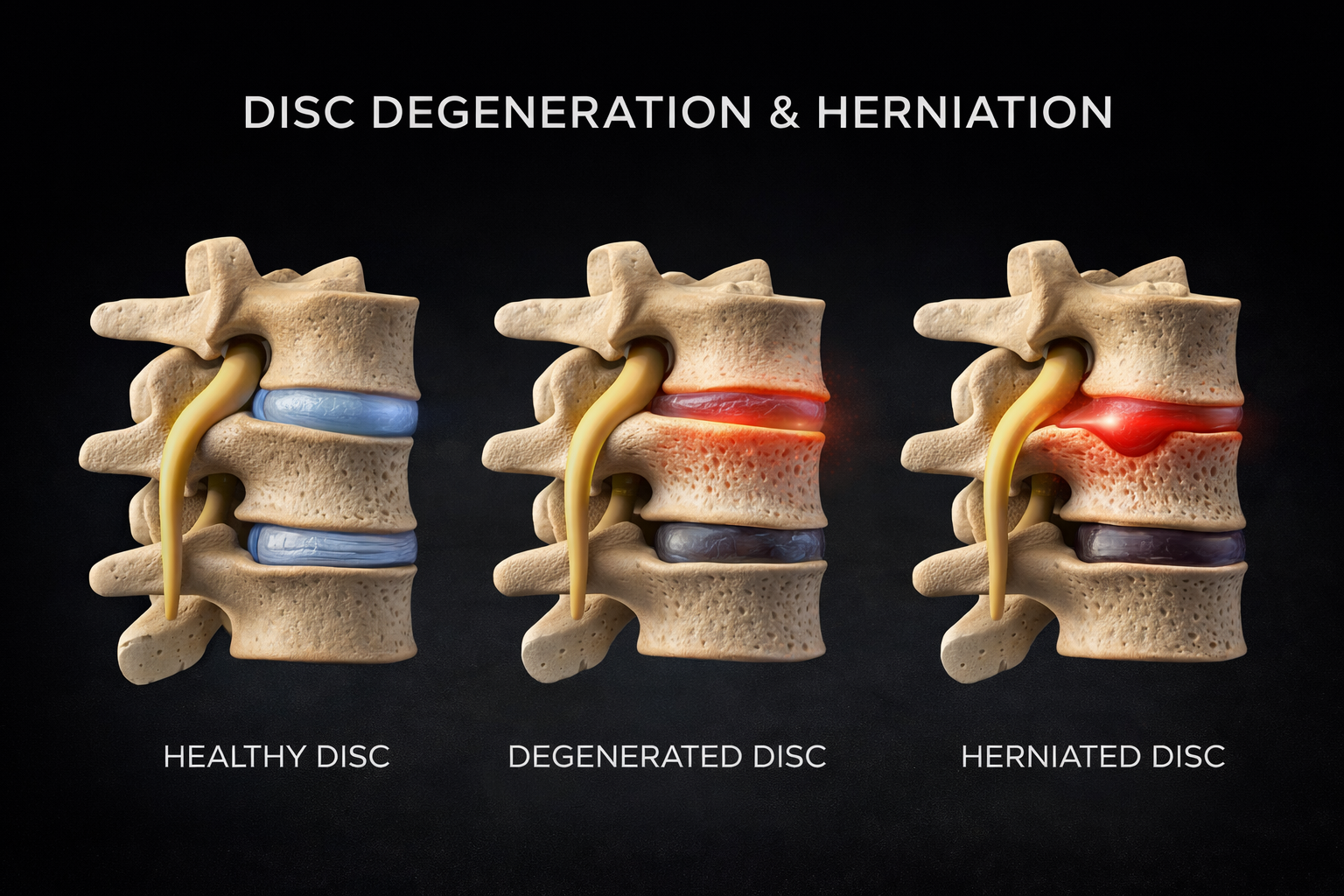
A disc herniation happens when part of an intervertebral disc—the cushion between the bones of your spine—begins to bulge or rupture. Discs have a tough outer ring (annulus fibrosus) and a gel-like center (nucleus pulposus). With stress, aging, or injury, the outer ring can weaken or tear, allowing the inner material to push outward.
A herniation can irritate nearby structures, especially spinal nerves, which may cause symptoms that travel into an arm or leg.
Common symptoms
Symptoms depend on the location and severity of the herniation and whether a nerve is irritated.
Local neck or back pain
Radiating pain (arm pain from the neck; leg pain/sciatica from the low back)
Tingling or numbness
Weakness in certain muscle groups
Pain worsened by sitting, bending, coughing, or sneezing
Seek urgent care if you have new bowel/bladder changes, saddle numbness, or rapidly worsening weakness.
What causes disc herniations?
Disc herniations are commonly linked to a combination of:
Repetitive bending/twisting or heavy lifting
Poor movement mechanics or prolonged sitting
Prior injury
Age-related disc dehydration and reduced resilience
Genetics and overall tissue health
How disc herniations affect movement
When a disc and surrounding tissues are irritated, your body often responds with muscle guarding and altered posture. This can reduce motion in the spine and shift load to other joints and muscles. Over time, these compensations can increase stiffness, reduce strength, and make everyday activities feel harder.
How they’re evaluated
A clinical evaluation typically includes:
History and symptom mapping
Neurological screening (strength, sensation, reflexes)
Movement assessment and special tests
Imaging (like MRI) is not always needed right away. Many disc herniations improve with appropriate conservative care and time, and imaging is most helpful when there are red flags, significant neurologic findings, or symptoms that don’t improve as expected.
Treatment approach
Most care plans focus on reducing irritation and restoring function:
Activity modification and education (what helps vs. aggravates)
Manual therapy to improve mobility and reduce protective tension
Targeted rehab to restore strength and stability
Nerve “mobility” strategies when appropriate
Gradual return to lifting, work, and sport
The goal is not just symptom relief—it’s improving movement capacity and reducing the chance of recurrence.